



Hip Fractures: Intertrochanteric, Subtrochanteric, and Femoral Neck
Aug 30, 2019Richard “Alex” Sweet II, MD
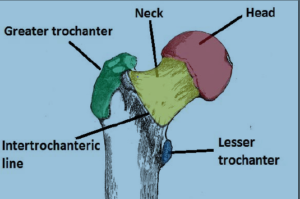
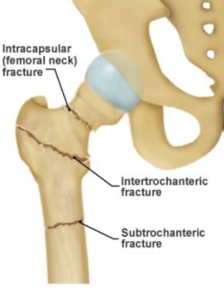
Anatomy: The femur (thigh bone) at the level of the hip is made up of 4 different parts: the head, neck, greater trochanter, and lesser trochanter. Fractures can occur anywhere within these 4 regions. Typically, isolated greater trochanteric fractures can be treated non-operatively. However fractures occurring between the greater and lesser trochanters, called Intertrochanteric Fractures do require surgery, as do fractures occurring below the trochanters known as Subtrochanteric Fractures. Femoral neck fractures also require surgery, but are treated differently as discussed later. Isolated femoral head or lesser trochanteric fractures are very rare. Despite the fact that all of these fractures occur in the “hip”, the treatment can vary widely based on the location of the fracture, the amount of displacement, and the health of the patient.
Intertrochanteric/Subtrochanteric Hip Fracture
Intertrochanteric fractures are the most common of all hip fractures. The fractures are rarely “clean” breaks and usually the bones have fairly significant comminution (fragmentation). They require surgical stabilization for healing. Surgery is performed by inserting a rod down the femur (thigh bone). Compression screws are then passed into the femoral neck and head to hold the fracture stable. One screw is also placed further down the thigh bone to lock in rotation of the hip fracture and provide stability. Postoperatively full weight is allowed on the hip.
- Dual screw system: Some hip fracture systems use a single screw for fixation of the fracture. The use of a second screws allows for superior stabilization of the fracture as well as the ability to compress the fracture. Compression stimulates the bone to heal faster and improved stability decreases postoperative pain during mobilization, making recovery faster and safer. This is why I almost always use this system for my patients.
- Post-Surgical Expectations: Most patients are allowed to “weight bear as tolerated” meaning that they can put as much weight down on the leg as pain will allow. While the hip is sore postoperatively, it is completely safe to bear weight and doing so compresses the fracture and promotes healing. Additionally, early mobilization prevents blood clots, pneumonia, bed sores, and other medical complications known to happen after hip fractures.
- Subtrochanteric Fracture: While these fractures are treated similarly, they are somewhat different. In general the surgery is much more challenging because aligning the bone back to its proper anatomical position is quite difficult. This often necessitates a larger incision. Like an intertrochanteric fracture, subtrochanteric fractures are treated with a rod, however the rod is usually much longer and sometimes goes all the way down to the knee.
Femoral Neck Fractures
These fractures are less straightforward. There are several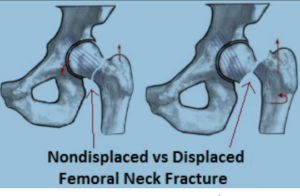 treatment options available and deciding on the best surgery is something that must be done on an individual basis. However I have tried to lay out my general guidelines and principles to help explain the rationale used.
treatment options available and deciding on the best surgery is something that must be done on an individual basis. However I have tried to lay out my general guidelines and principles to help explain the rationale used.
- Nondisplaced: The first thing that must be determined is, how bad is the fracture. When the femoral neck breaks, the head can completely separate from the neck, or it can remain relatively well aligned. Nondisplaced fractures typically can be treated with screw fixation. Three large screws are passed through the fracture site to compress the fracture and hold it in place. After surgery, 50-100% weight bearing may be allowed depending on the patient and the fracture. Unfortunately these surgeries do have a significant failure rate and I tend to recommend this surgery only in very sick, less active, and extremely elderly patients.
• Displaced: The femoral head has a very delicate blood supply. If the head displaces from the neck then the blood supply has been ripped apart. While realigning the bone and fixing the fracture is always possible, the fracture cannot heal with its blood supply gone. The hip will likely fail. These fractures cannot be fixed and instead must be replaced. Even in nondisplaced fractures the blood supply can be compromised, leading to a high failure rate of screw fixation surgery.
› Partial Hip Replacement (Hemi-arthroplasty): This is the traditional treatment for displaced femoral neck fractures. It involves replacing the head and neck bone with a metal prosthetic. This treatment is a slightly faster procedure, moderately less complex and the complication rate is a few tenths of a percentage lower than a full hip replacement. The ease of this procedure has made it the gold standard for elderlypatients with displaced femoral neck fractures.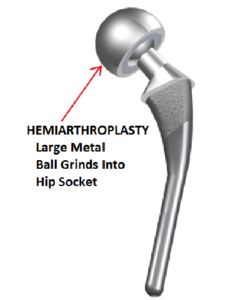
› Total Hip Replacement (Total Hip Arthroplasty): This is one of the most successful (if not the MOST successful surgery) in all of the surgical fields. In terms of patient satisfaction and outcomes, few surgeries can rival a total hip replacement. With the advent of the minimally invasive anterior approach this surgery has become an even better option for many patients. The biggest advantage of the total hip is in the replacement of the acetabular cup (socket part of the ball
and socket joint). This allows for a bearing surface for the femoral head. In a hemiarthroplasty the metallic femoral head grinds into the cartilage of the acetabulum and can wear it out fast, causing potentially severe pain and disability. The total hip eliminates this complication. While this surgery is not right for all patients and should not be performed by all surgeons, as a fellowship trained hip and knee replacement specialist, I can offer this highly specialized surgery with a relatively low risk profile.
Expected Outcome: Hip fractures are devastating injuries and results vary widely based more on the health of the patient and less on the fracture. Very elderly and sick patients that suffer a hip fracture can take a long time (up to a year) to recover. The hip is rarely the problem, rather it is the heart, lungs, kidneys and the rest of the body struggling to recover from the trauma. Healthier patients that just happened to have a hard fall (that caused the fracture), but are otherwise active and healthy for their age, are expected to do much better. There is a great deal of variability and it is near impossible to predict the outcome before surgery. Most patients need at least 3-7 days in the hospital followed by a stay in a nursing home or SNF facility. Additionally, most patients lose some mobility post op, and require more assistance than before the injury.





 Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics.
Our patients can receive MRI imaging onsite at both our Louisville and New Albany Clinics. Providing the latest advances in orthopedic surgery is our specialty.
Providing the latest advances in orthopedic surgery is our specialty. We take a unique, multidisciplinary approach to pain management.
We take a unique, multidisciplinary approach to pain management. Our physical therapists use advanced techniques to help restore strength and mobility.
Our physical therapists use advanced techniques to help restore strength and mobility.  We provide comprehensive, conservative care for a wide variety of foot and ankle conditions.
We provide comprehensive, conservative care for a wide variety of foot and ankle conditions. We offer same- and next-day care to patients with acute injuries.
We offer same- and next-day care to patients with acute injuries. Get back in the game with help from our sports medicine specialists.
Get back in the game with help from our sports medicine specialists.  Our centers are equipped with a state-of-the-art digital X-ray machine.
Our centers are equipped with a state-of-the-art digital X-ray machine.